First Zygomatic Implant Surgery In Sri Lanka Performed in May 2024
A Milestone in Sri Lankan Dentistry: The First Zygomatic Implant procedure
Pioneering Dental implant Surgery: Performing the First Zygomatic Implant Surgery in Sri Lanka: May 2024. By Dr Hirantha Weragoda.Welcome to my blog, Dedicated to the advanced procedures, I’m introducing in Sri Lanka -Like the countries, The first Zygomatic Implant surgery was performed(May 2024)at LIMDENT Surgical, Dental Hospital, and Full mouth reconstruction with multi unit abutment (May 2024) and Leading the way in Sri Lanka. I’ve embraced the future of dentistry with state of the art digital technology and precise implant planning design. Moreover, this blog will help by the facts and art of overcoming any complicated challenges in dentistry.
The historical clinical case in Sri Lankan Dentistry
Clinical Case
A 65 year old male presented with failed conventional implants and resorbed jawbones, requesting a permanent solution. With insufficient bone for traditional methods, I determined the most effective course of action was the renowned zygomatic approach, marking a new milestone in Sri Lankan dentistry.
A thorough examination was paramount, leading to CBCT scans for precise bone assessment and digital smile designing photos to craft a comprehensive plan. Intraoral photographs captured detailed evidence of the pre operative conditions. Intra Oral Scanning was done mainly for the purpose of digital treatment planning, Surgical implant guide fabrication and the other advanced procedures for the full mouth reconstruction. Take a look at the CBCT imaging and the initial photos that guided our approach.
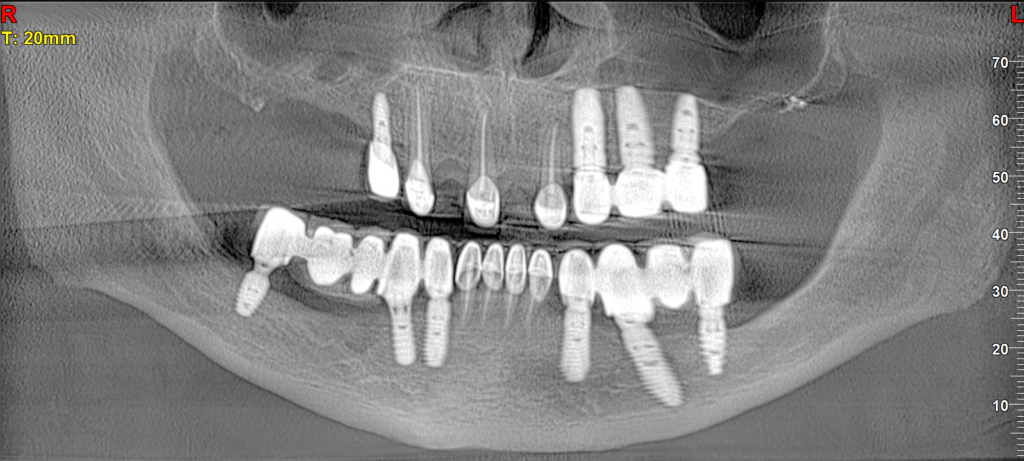


Figure 2 ; “Pre-operative frontal intraoral view demonstrating the clinical status of the existing prosthesis and soft tissue.”Figur 3 ;“Maxillary occlusal view showing severe alveolar ridge resorption and the limited bone volume available for conventional implants.”
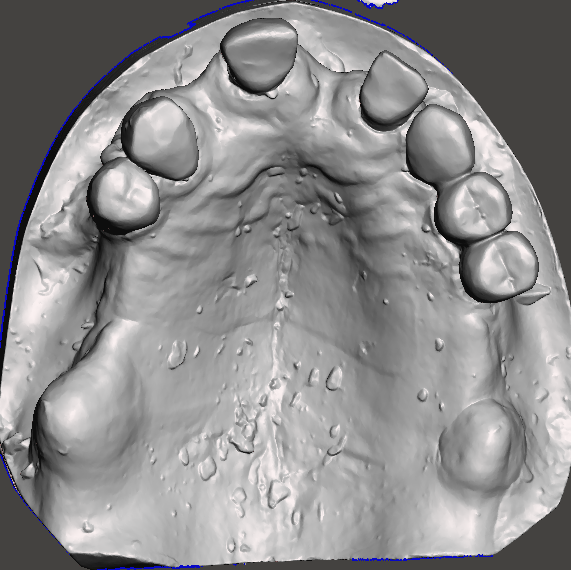
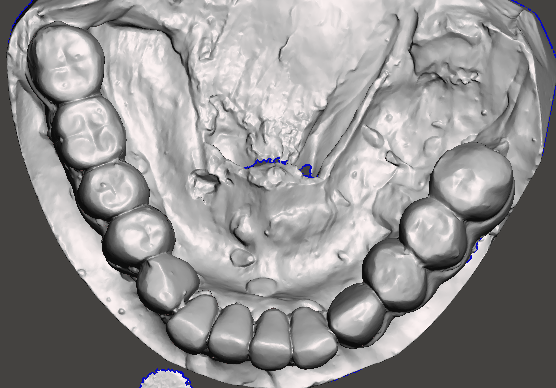
“Digital treatment planning: 3D intraoral scans of the maxillary and mandibular arches used for precise virtual implant positioning and surgical guide fabrication.
Treatment planning
I completed pre operative planning for the implant placement utilizing surgical guide software, Integrating CBCT and intraoral scan data for virtual planning and maximum precision. Leveraging digital planning technology, I engineered surgical guides for both zygomatic and conventional implants, alongside bone reduction and pin guides and developed a guide for the temporary prosthetics using implant planning software.
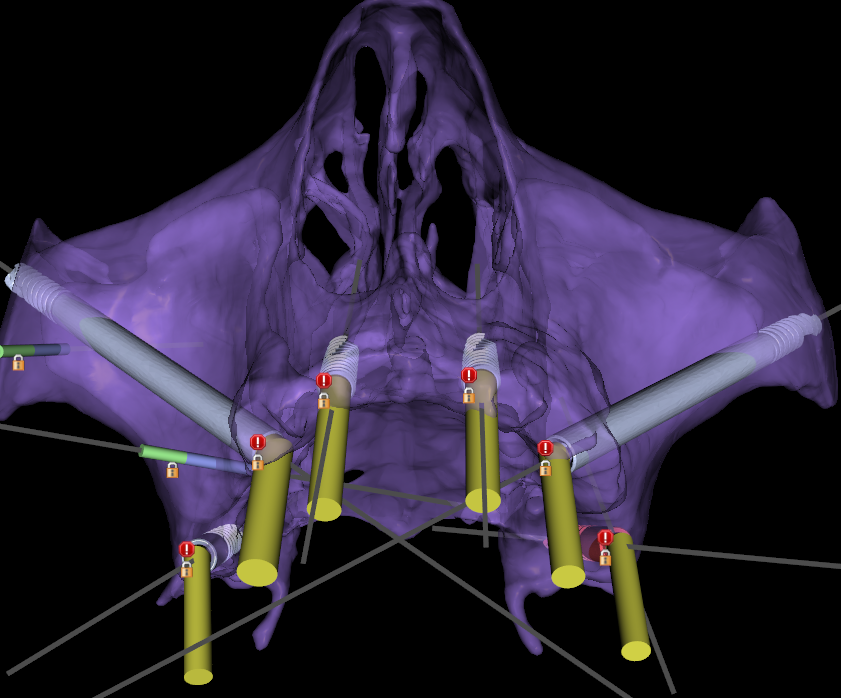
“Precision Digital Planning: 3D mid-face skeletal reconstruction and implant simulation designed using Blue Sky Bio software. This virtual model features a complex 6-implant configuration—including 2 zygomatic and 2 pterygoid implants—to ensure optimal anatomical anchorage and surgical accuracy.”
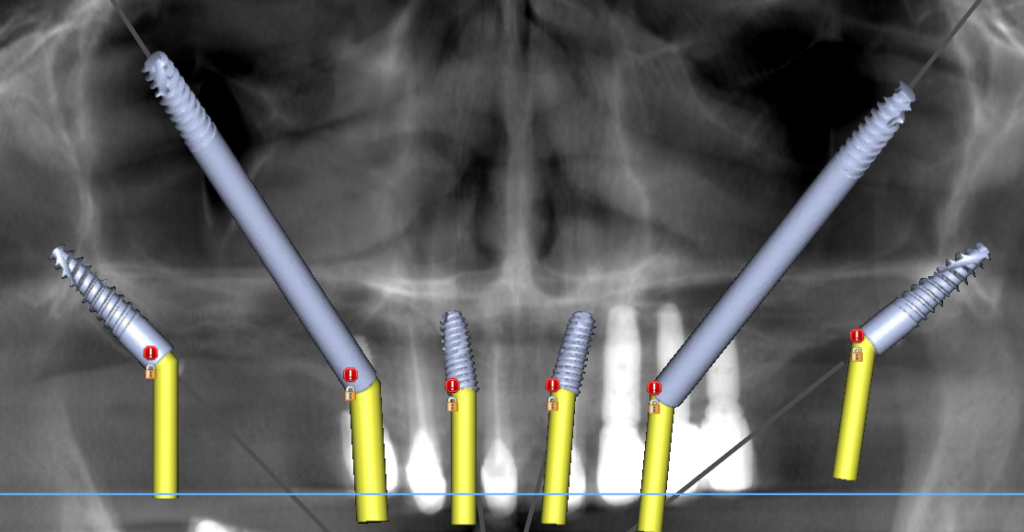
“2D Surgical Simulation: Panoramic treatment planning designed in Blue Sky Bio software, visualizing the strategic distribution of zygomatic, pterygoid, and conventional implants for maximum primary stability.”

From left to right; Immediate loading upper temporary prosthesis, Left zygomatic implant osteotomy surgical guide, right zygomatic implant osteotomy surgical guide, upper pin guide, upper pterygoid surgical guide.
Surgery

Pictures from let to right; Zygomatic depth probe guiding the trajectory of the osteotomy, First Zygomatic implant is being driven in to the zygomatic bone in history of Sri Lanka by Dr Hirantha Weragoda. First Zygomatic implant in history of dentistry in Sri Lanka in place May 2024.

Surgical site was closed with 4/0 non absorbable suture, After Right and left Zygomatic implants, Pterygoid and anterior conventional implants being placed.
Surgery was performed under IV sedation anaesthesia under a supervision of an Specialist anaesthetist in combination with local anaesthesia. The total surgical time took from the introduction of anaesthesia to the wound closure was 6 hours. Lignocaine with adrenaline in concentration of 1:80000 was used to anaesthetize the upper and lower jaws respectively maxillary anterior middle and posterior and incisive nerves. Lower bilateral inferior dental nerves and long buccal nerves. Then Marcaine with dexamethasone was used to top up locally to enhance and prolong the anaesthetic effect.
First pin guide was used and then buccal and palatal full thickness flaps were raised. Palatal flap was kept away from the alveolar bone by and anchoring suture. Anterior vertical incision was done and extended to facilitate the extension of the buccal flaps to expose the lateral wall of the maxillary antrum and the anterior segment of the zygomatic bone. Standing teeth and the previous implants were removed carefully preserving the alveolar bone. Left upper implants in the premolar region were kept behind avoid the unnecessary damage of the alveolar bone. Alveolar bone was planed and levelled by bone reduction as planned pre-operatively. Implant insertion was bone one side at a time due to the convenance. Fist, pterygoid implant was done with the guidance of the surgical guide. Then zygomatic implant was done. Using the zygomatic surgical guide, the trajectory was made according to the plan. This was intra-maxillary approach in left side and extra-maxillary approach right side zygomatic implant placement.
Mandibular implants were done in the same way with using a surgical guide.

“Mandibular Reconstruction: Precision placement of 6 mandibular implants achieved through a fully guided surgical workflow. The use of a custom surgical guide ensured optimal implant positioning and parallelism, providing a stable foundation for the lower prosthesis.”
After, all the implants being inserted, alveolar bone was further shaped and smoothed with the burr and teeth extraction sockets and other bone defects were repaired with the paste made with harvested bone from the patient, synthetic bone graft and PRF/PPP extract form the patient’s blood.

All the implants were loaded with the multi-unit abutments(MUA) according to the planned angulations. Then the site was closed with 4/0 nonabsorbable suture leaving the MUA exposed.
Temporary prosthesis was not loaded due the extended time of the surgery and planned it for the delayed loading after a week post operatively.

“Post-operative radiographic assessment: The OPG (top) and 3D CT reconstruction (bottom) confirm the accurate placement of the maxillary and mandibular implants, demonstrating excellent primary stability and alignment according to the pre-surgical digital plan.”
Prosthetic Phase
There are three main prosthetic phases to achieve the final permanent prosthesis.
- First temporary prosthesis, delayed loading. Upper 3D-Prinded resin full arch, and Lower modified acrylic denture.
- Two months post operatively, Intermediate upper and lower prosthesis were made.
- Final permanent prosthesis, 6 months post operatively.

“The intermediate phase: A 3D-printed PMMA provisional bridge for the upper arch and a modified acrylic denture for the lower. These temporary prostheses allow the patient to maintain function and aesthetics while the implants undergo osseointegration before the final restorations are fabricated.”

“The definitive upper restoration: A monolithic full zirconia bridge for superior aesthetics and wear resistance, supported by a CAD/CAM milled titanium bar. The use of a titanium substructure with precision-milled abutment cylinders ensures a passive fit and long-term structural integrity for the full-arch implant reconstruction.”

“The definitive lower prosthesis: A monolithic zirconia full arch bridge utilizing Ti-base technology. This approach combines the high-strength and aesthetic properties of zirconia with the precision-engineered fit of titanium bases, ensuring optimal soft tissue response and long-term prosthetic stability.”
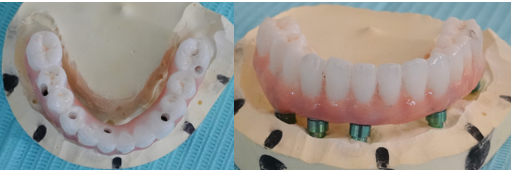
“Laboratory verification: The final monolithic zirconia mandibular bridge is shown here fitted on the master model. This stage is crucial for confirming the passive fit of the Ti-base connections and ensuring the occlusal anatomy and emergence profiles meet the exact specifications of the digital design before clinical delivery.”
Final Prosthesis


BEFORE AFTER
Conclusion
This landmark surgery, performed pioneeringly in Sri Lanka, marks a triumphant fusion of surgical precision, patient trust, and unwavering team brilliance. It’s not just the first zygomatic surgery in the nation history, but also a successful integration of the most advanced digital technologies. By seamlessly combining state of the art digital smile design precise implant placement guided by multiple surgical guides an expert prosthetic planning, this case sets a new standard for comprehensive rehabilitation. Spanning six continuous hours, it successfully harnessed guided surgery for implants, elevating precision and predictability, the customs surgical guides utilized in this case were designed not just for conventional implants but also were successfully applied to both zygomatic and Pterygoid placements. And employed the latest digital treatment planning for state of the art full mouth reconstruction. From the initial temporary prosthesis to the final design, every phase, including milling with advanced technology, moved towards the desired prosthetic outcome. It’s success stands as a treatment to the power of innovation and dedication, illuminating a path forward for complex rehabilitation.
"Dr. Hirantha Weragoda, BDS (Hons), is a specialized Dental Surgeon with expertise in Implants, Oral Surgery, Zygomatic implants, and Full mouth reconstruction in Sri Lanka. Graduating with Honors, Dr. Weragoda is committed to clinical excellence and advanced dental solutions."
View All Articles